

Which Of These Values Changes The Most During Mild To Moderate Exercise?
Introduction [edit | edit source]

Therapeutic exercise involves movement prescribed to correct impairments, restore muscular and skeletal role and/or maintain a land of well-being[1]. The scientific evidence demonstrating the beneficial effects of exercise is indisputable, and the benefits of exercise far outweigh the risks in well-nigh adults. For most adults, an do plan including aerobic, resistance, flexibility, and neuromotor practice training is indispensable to improve and maintain concrete fitness and health[2].
Therapeutic exercise a cadre skills upon which the profession of physiotherapy is based. How does exercise differ from physical activity? [three].
- Concrete activity refers to the contraction of skeletal musculus that produces bodily movement and requires energy.
- Exercise is a concrete activity that is planned and is performed with the goal of attaining or maintaining concrete fettle. Concrete fitness is a prepare of traits that allows an individual to perform physical activeness[4].
Types of exercises [edit | edit source]

Therapeutic exercise may include:
- aerobic and endurance conditioning and reconditioning
- agility preparation;
- body mechanics preparation;
- animate exercises;
- coordination exercises;
- developmental activities grooming;
- move pattern training;
- neuromotor development activities training;
- neuromuscular didactics or reeducation;
- perceptual preparation;
- range of movement exercises and soft tissue stretching;
- relaxation exercises;
- strength, power, and endurance exercises.[v]
The most normally included exercises fall into 4 groups
- Strengthening exercises, normally performed with heavy resistance and fewer repetitions.
- Endurance exercises that engage large muscle groups over a longer period of time, in the area of fifty to sixty% VO2Max to accomplish greater cardiovascular endurance[ane].
- Flexibility exercises achieved through stretching and move.
- Balance and coordination exercises that focus on maintaining an individual's middle of gravity.
All of these are combinable into exercise programs that work for many different types of patients. Different subtypes of exercises can help to increase effectiveness or allow participation of individuals with special needs based on comorbidities. eg. aquatic therapy for stroke patients with balance difficulties
Basic exercise prescriptions should follow the FITT mnemonic.
F- frequency: number of days per week
I- Intensity: low, moderate or vigorous
T- Time: minutes per session for endurance exercise
T- Type: endurance, forcefulness, flexibility or some combination[5]

Endurance Exercises [edit | edit source]
The dose of exercise can be described using the so-called FITT factors, where FITT stands for Frequency, Intensity, Time, and Blazon of activity[6].
Frequency (how often)
Practice should exist carried out iii-five days a week.
Training three times a week produces significant training furnishings; however, training 5 days a calendar week at a lower-intensity exercise may be more manageable for some people. Footling additional do good is seen with more than v training sessions a calendar week, and the take a chance of injury is increased. Training twice a week does not produce increases in VO2max; however it may produce some functional changes and information technology is probably better than no exercise at all[3].Moderate intensity aerobic exercise done at least 5 d ∙ wk or vigorous intensity aerobic exercise done at to the lowest degree 3 d ∙ wk or a weekly combination of three–5 d ∙ wk of moderate and vigorous intensity exercise is recommended for most adults to reach and maintain health/fitness benefits[7].
Intensity (how difficult)
Intensity refers to the rate at which the action is existence performed or the magnitude of the endeavor required to perform an activity or exercise. It can be thought of "How hard a person works to do the activity".Intensity tin be monitored by heart rate in almost patients, although some patients may accept pathology or be on drug handling that affects their HR response to practice in which case HR cannot be used to monitor practice intensity. Exercise is categorized into three different intensity levels. These levels include low, moderate, and vigorous[3].
The overload principle of training states that exercise below a minimum intensity, or threshold will non challenge the trunk sufficiently to result in changes in physiologic parameters, including increased maximal volume of oxygen consumed per unit of fourth dimension (VO2max)[7].
The Karvonen method, which takes into account resting can be used to calculate an individual's training HR band using the following adding. A method of calculating the training heart rate, which is equivalent to a desired percent VO2max. Information technology involves adding a given percentage of the maximal middle charge per unit reserve (maximal centre charge per unit—resting eye rate) to the resting eye rate. The maximal heart rate is commonly assumed to exist 220—age in years. Therefore, the following equation is used to calculate the preparation heart rate for a work rate equivalent 75% VO2max: training centre rate = 0.75 max HRR + resting 60 minutes; where max HRR is the maximum Heart Rate Reserve, and resting HR is resting Heart Rate. A target center rate range for grooming is commonly fix at values of betwixt 50 and 85% of VO2max, i.e. 0.50 × max HRR + resting HR to 0.85 max HRR + resting Hr[viii].
[9]
In the absence of a heart rate monitor people tin can monitor their ain pulse to ensure that they are working at the correct intensity. Patients should be taught how to accept their carotid pulse within the first 10 or fifteen seconds of terminating practice and multiplying up the beats counted past 6 or iv respectively to provide beats per minute. Oxygen uptake tin can too exist used to gear up exercise intensity, and an intensity of twoscore-50% to 85% of the oxygen uptake reserve is recommended.
Measures of perceived effort and melancholia valence (i.e.the pleasantness of exercise) tin be used to attune or refine the prescribed exercise intensity. These measures include the Borg Rating of Perceived Exertion (RPE) Scales,OMNI Scales,Talk Test and Feeling Scale[vii].
Walking is the most common class of endurance practise practiced and it is the 1 almost frequently recommended by doctors. Walking can be easily incorporated into the daily schedule. One study showed that seniors who walk at to the lowest degree 2 miles a day on average lower their mortality risk by 50 per centum. Other good forms of endurance grooming are swimming, cycling, dancing, walking up stairs instead of taking the elevator, golf game (walking), gardening or heavy yard work, and low-impact aerobics.[ten]
Time (duration or how long)
A total of 20-60 minutes of continuous or intermittent aerobic activeness a mean solar day should be performed. The activity can exist divided into a minimum of lO-minute bouts throughout the 24-hour interval. The duration of preparation is dependent on the intensity. Individuals starting at the lower end of the preparation band demand to sustain practise longer (xxx-60 minutes) to achieve grooming effects[3].
Blazon
Rhythmic, aerobic exercise of at least moderate intensity that involves large muscle groups and requires lilliputian skill to perform is recommended for all adults to improve health and CRF. Other exercise and sports requiring skill to perform or college levels of fitness are recommended only for individuals possessing adequate skill and fettle to perform the activity[seven].
Strengthening Exercises [edit | edit source]
Strength grooming is done to build up muscle tissue; it typically consists of graded exercises involving resistance preparation. Strength preparation may be high or moderate in intensity.[10]
This modality increases overall strength and comes in three forms: isotonic, isometric, and isokinetic.
- Isotonic consists of dynamic movements with a constant load.
- Isokinetic involves a abiding velocity with variable load.
- Isometric involves muscle contraction that is static with no modify in muscle length.
Resistance training (RT) has been acknowledged as an effective method to amend muscular strength, ability, and hypertrophy which are key components of physical fitness related to the quality of life[11].Traditional resistance training recommendations propose an intensity of 60–70% 1 repetition maximum (1 RM) in novice exercisers to ameliorate strength[12]. Compared to no do, however, loads beneath threescore% one RM tin can also induce significant strength gains in older good for you adults. An exercise training program ideally is designed to meet individual health and concrete fettle goals within the context of private wellness status, function, and the respective physical and social surround[13].
For adults of all ages, the goals of a wellness-related resistance training programme should beto (a) make activities of daily living (ADL) (e.one thousand., stair climbing, carrying numberless of groceries) less stressful physiologically and (b) finer manage, attenuate, and even prevent chronic diseases and health weather condition such as osteoporosis, Type two diabetesmellitus, and obesity. For these reasons, although resistance preparation is important acrossthe historic period span, its importance becomes even greater with age[7].
Load dosage
ACSM recommends:
- Frequency -ii-3 days a week, but in other scientific bespeak of view these frequency recommendations are however notional, derived from conjecture rather than robust scientific evidence. This lack of prove weakens established recommendations regarding progressive RT loading and training volumes for improved muscular forcefulness[14].Several RT studies have reported that an RT frequency of two to 3 days calendar week− 1 for previously untrained individuals produces optimum strength gains[15].Feigenbaum and Pollock suggest that a single prepare program of xv repetitions performed at a frequency of ii to three days week− 1 allows for sufficient regeneration, while still providing fourscore–90% strength gains of more frequent RT programs. Moreover, the authors suggest that each RT session should be comprised of 8 to x different exercises that target the major muscles. However, these recommendations are generalised and are provided for all subjects with varying health conditions and age ranges[16]. RT studies frequently cited in scientific literature do not fairly describe the frequency for different population groups (untrained, trained, and well trained)[17].
- Intensity - percent of i RM e.one thousand. 73% of 1RM[eighteen].
- Elapsing -3 seconds for the concentric phase and 3 seconds for the eccentric phase of the activity (about 1 minute in total).
- Volume -number of sets and repetitions[xviii].


Flexibility Exercises [edit | edit source]
Flexibility training: slowed, controlled exercises performed in a gradual manner (commonly in the increment of fifteen to thirty seconds) that aid in the range of motion at joints or series of joints. 3 master types exist: static, dynamic, and PNF (proprioceptive neuromuscular facilitation).
- Static involves held positions that are effective with piffling required in terms of help and time.
- Dynamic involves repetitive bouncing movements that produce muscle stretch over time.
- PNF involves alternating wrinkle and relaxation of agonist/antagonist muscles at specific joints that by and large produce the largest increment in flexibility.[1]

Balance and Co-ordination [edit | edit source]
Optimal control of balance in an upright stance is an essential requirement for sport, daily activities, and prevention of injury[19]. For example, dumb postural control is associated with an increased take a chance of ankle sprain[20]. Considering of this strong association, residuum and coordination training are mutual components of condom and therapeutic intervention programs used by athletic trainers and other health care providers to treat patients with a variety of musculoskeletal conditions. Moreover, mounting testify demonstrates that various residual-training programs improve postural control[21]and reduce the recurrence of musculoskeletal[20]. injuries (eg, ankle sprains)
Despite the effectiveness of balance training in improving these outcomes, the verbal parameters needed to maximize the benefits of balance-training programs remain unknown. One factor that has gained involvement of tardily is the progression fashion. For instance, participants or patients could exist progressed to higher difficulty levels within a balance-training program after a set amount of fourth dimension at a particular level (eg, 2 sessions or 8 repetitions). In contrast, participants or patients could be progressed only later on they take demonstrated consistent movement proficiency. Some testify suggests that balance improves when using a time-based or repetition-based–progression manner[22].
According to the dynamic systems theory, an error-based progression style that evaluates consistent motion proficiency would let the sensorimotor system to cocky-organize around a given set of chore and ecology constraints earlier being challenged with greater demands at a higher difficulty level, which could issue in a more profound comeback[23]. Nevertheless, individual differences in the rate of cocky-organization and motility proficiency for a given task could vary significantly and thus may be a reason why this progression style has not been investigated empirically until recently. Indeed, several groups of researchers studying persons with chronic ankle instability (CAI) demonstrated that an error-based balance-preparation program was effective in improving postural control[24]e.grand. McKeon et al study showed neat results, 12 supervised preparation sessions, lasting about 30 minutes each over a 4-week period[24].

Physiotherapy [edit | edit source]
At that place is strong evidence that aerobic exercise (xl-50% HRR progressing to 60-80%) conducted twenty-40 min and 3-5 days per week is beneficial for enhancing aerobic fettle, walking speed and walking endurance in people who have had balmy to moderate stroke and are deemed to accept low cardiovascular risk with do after proper screening assessments[25].
Ix manufactures (seven RCTs) were identified. The exercise intensity ranged from fifty% to eighty% center charge per unit reserve. Exercise duration was twenty-40 min for 3-v days a week. The total number of subjects included in the studies was 480. All studies reported positive furnishings on aerobic capacity, regardless of the stage of stroke recovery. There is skillful bear witness that aerobic practise is beneficial for improving aerobic capacity in people with mild and moderate stroke. Aerobic do should be an important component of stroke rehabilitation[26].
C. Liebenson for back pain recommends Stability Training Variables
- Intensity: submaximal, less than fifty% of single repetition maximum (1RM)
- Sets and repetitions: starting time with one set of approximately six repetitions
- Progress to ane set of 12 repetitions
- Further progress after the reverse pyramid arroyo of add i ng a second set o f 8 repetitions,and and then a third prepare of iv reps
- Hold times: emphasize endurance by holding for i to ii breaths (6 to one 0 seconds)
- Course : movements should be performed slowly with advisable form for motor control training and injury prevention
- Frequency: daily or twice daily to im show motor command
- Duration: up to iii months required to re-brainwash movement patterns in a patient with chronic pain
- The variables in stability tra i north i ng include i n tensity,sets, repetitions, concord times, grade, frequency, and elapsing[27].
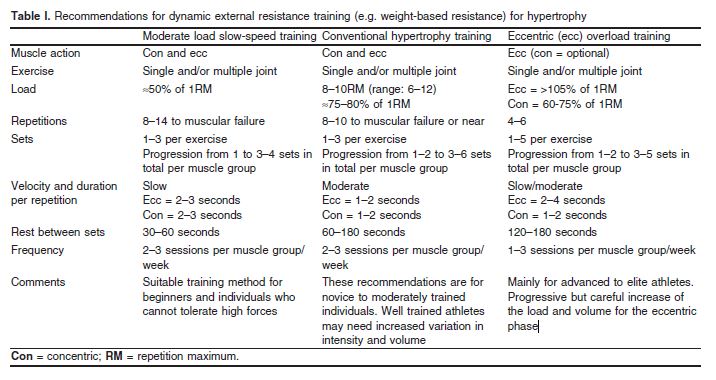
Wernbom M, et all recommends dynamic external resistance grooming (e.one thousand. weight-based resistance) for hypertrophy[xviii].
Principles of exercises for chronic not-inflammatory diseases and others wait here.
For cardiac and pulmonary rehabilitation, there is an interprofessional requirement for Physical therapists, occupational therapists, and all levels of clinical involvement due to the acuity of patients involved.
For individual sports injuries, only physical therapists may be necessary to guide the patient through specific regimens. Incorporating abode exercises that are easy and safe to perform lonely allows peripheral surveillance with minimal risk.[1]
References [edit | edit source]
- ↑ one.0 1.1 i.2 1.three Bielecki JE, Tadi P. Therapeutic Do. StatPearls [Internet]. 2020 Mar 19.
- ↑ Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, Nieman DC, Swain DP. American Higher of Sports Medicine position stand up. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Medicine and science in sports and practise. 2011 Jul one;43(7):1334-59.
- ↑ 3.0 three.one 3.ii 3.3 Glynn A, Fiddler H.The Physiotherapist's Pocket Guide to Exercise Assessment, Prescription and Training,Churchill Livingstone, 2009.
- ↑ Eric H, Gary J. Exercise and the Centre.Cardiology Secrets (Third Edition)2010, Pages 311-315
- ↑ 5.0 5.i Guide to do. Therapeutic exercise Bachelor from:http://guidetoptpractice.apta.org/content/one/SEC40.extract (terminal accessed 24.5.2020)
- ↑ Takken T, Giardini A, Reybrouck T, Gewillig 1000, Hövels-Gürich HH, Longmuir PE, McCrindle BW, Paridon SM, Hager A. Recommendations for physical activity, recreation sport, and do preparation in paediatric patients with congenital heart disease: a report from the Practice, Basic & Translational Research Section of the European Association of Cardiovascular Prevention and Rehabilitation, the European Built Centre and Lung Exercise Group, and the Association for European Paediatric Cardiology. European journal of preventive cardiology. 2012 October 1;xix(5):1034-65.
- ↑ 7.0 7.ane 7.2 seven.3 7.4 American College of Sports Medicine.ACSM's Guidelines for Exercise Testing, 2017.
- ↑ Kent M.The Oxford dictionary of sports science and medicine,Oxford Academy Printing, 2007 - 612 p.
- ↑ Neil Bergenroth: Rowing Double-decker. How to Calculate Heart Charge per unit Intensity. Bachelor from: https://https://www.youtube.com/lookout man?five=09BqXAEvtBc[final accessed 27/6/2020]
- ↑ x.0 ten.1 Encyclopedia Therapeutic exercises Available from:https://www.encyclopedia.com/caregiving/encyclopedias-almanacs-transcripts-and-maps/therapeutic-exercise (last accessed 25.4.2020)
- ↑ Hunter GR, McCarthy JP, Bryan DR, Zuckerman PA, Bamman MM, Byrne NM.Increased forcefulness and decreased flexibility are related to reduced oxygen cost of walking.Eur J Appl Physiol. 2008 November; 104(5):895-901.
- ↑ Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, Nieman DC, Swain DP, American College of Sports Medicine. American College of Sports Medicine position stand. Quantity and quality of practice for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011 Jul; 43(seven):1334-59.
- ↑ Garber CE, Blissmer B, Deschenes MR, et al. American College of Sports Medicine position stand up. The quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in obviously salubrious adults:guidance for prescribing practise. Med Sci Sports Exerc. 2011;43(7):1334–59.
- ↑ Carroll TJ, Abernethy PJ, Logan PA, Hairdresser M, McEniery MT.Resistance training frequency: force and myosin heavy chain responses to two and three bouts per week.Eur J Appl Physiol Occup Physiol. 1998 Aug; 78(3):270-5.
- ↑ Braith RW, Pollock ML, Lowenthal DT, Graves JE, Limacher MC.Moderate- and high-intensity exercise lowers blood pressure in normotensive subjects sixty to 79 years of age. Am J Cardiol. 1994 Jun 1; 73(15):1124-8
- ↑ Feigenbaum MS, Pollock ML.Prescription of resistance grooming for health and disease. Med Sci Sports Exerc. 1999 Jan; 31(1):38-45.
- ↑ Grant W. Ralston, Lon Kilgore, Frank B. Wyatt,Duncan Buchan,and Julien South. Baker.Weekly Grooming Frequency Effects on Strength Gain: A Meta-Analysis.Sports Med Open. 2018 December; 4: 36.
- ↑ 18.0 18.ane xviii.2 Wernbom M,Augustsson J, Thome´e R. The Influence of Frequency, Intensity, Book and Mode of Strength Training on Whole Musculus Cross-Exclusive Area in Humans.Sports Med 2007; 37 (3): 225-264
- ↑ Anderson Grand, Behm DG.The impact of instability resistance training on residuum and stability. Sports Med. 2005; 35(1):43-53.
- ↑ xx.0 20.1 McHugh MP, Tyler TF, Mirabella MR, Mullaney MJ, Nicholas SJ.The effectiveness of a residual training intervention in reducing the incidence of noncontact ankle sprains in high school football players. Am J Sports Med. 2007 Aug; 35(8):1289-94
- ↑ Filipa A, Byrnes R, Paterno MV, Myer GD, Hewett TE. Neuromuscular training improves performance on the star excursion balance exam in young female athletes. J Orthop Sports Phys Ther. 2010 Sep; 40(ix):551-eight.
- ↑ Rothermel SA, Hale SA, Hertel J, et al. Effect of agile foot positioning on the outcome of a balance training plan.Phys Ther Sport. 2004; 5 2: 98– 103
- ↑ McKeon PO. Cultivating functional variability: the dynamical-systems arroyo to rehabilitation.Athl Ther Today. 2009; 14 iv: i– 3.
- ↑ 24.0 24.1 McKeon PO, Ingersoll CD, Kerrigan DC, Saliba E, Bennett BC, Hertel J.Balance grooming improves function and postural control in those with chronic ankle instability. Med Sci Sports Exerc. 2008 Oct; 40(10):1810-9.
- ↑ Pang MY, Charlesworth SA, Lau RW, Chung RC. Using aerobic do to improve health outcomes and quality of life in stroke: evidence-based practice prescription recommendations. Cerebrovascular Diseases 2013; 35(1): vii-22.
- ↑ Marco Y C Pang i, Janice J Eng, Andrew S Dawson, Sif Gylfadóttir. The Utilize of Aerobic Exercise Grooming in Improving Aerobic Capacity in Individuals With Stroke: A Meta-Analysis. Clin Rehabil. 2006 February;20(two):97-111
- ↑ Liebenson C. Rehabilitation of the Spine: A Practitioner'south Manual Second Edition; LWW; Second edition, 2006.

Source: https://www.physio-pedia.com/Therapeutic_Exercise
Posted by: carignangatellicited99.blogspot.com
0 Response to "Which Of These Values Changes The Most During Mild To Moderate Exercise?"
Post a Comment